Gold or platinum weight insertion: an incision is placed in the upper eyelid crease, and the cartilaginous portion of the eyelid is identified. A thin gold or platinum weight is then inserted into this space and centered over the cornea. It is secured with sutures to prevent migration, and the incision is closed. The amount of weight to be used is determined preoperatively by applying small weights to the upper eyelid.
Palpebral spring placement: an incision is placed in the upper eyelid crease, and a specially-designed spring is inserted. A tunnel is created for placement of the second limb of the spring near the eyebrow. The spring is the secured in place with sutures and tested during surgery with the patient awake. Blinking is performed, and the spring adjusted as necessary.
Levator palpebrae lengthening: an incision in the upper eyelid crease is placed, and the levator mechanism of the upper eyelid (responsible for elevating the upper eyelid) is identified. An opening in the mechanism is made. A piece of fascia graft is then taken from the temple region with dimensions corresponding to the degree of upper eyelid asymmetry (determined preoperatively).
Lower eyelid correction can also be achieved in a number of ways:
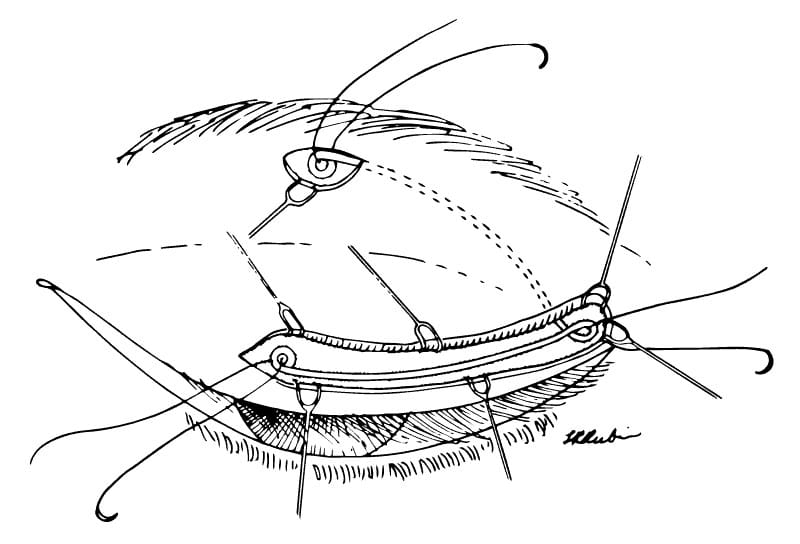
Lower eyelid tendon sling: small incisions are placed along the lower eyelid, and a small tunnel is created at the margin. A thin tendon graft is obtained, most commonly from the wrist, and transferred to the lower eyelid incisions. The tendon is then looped around the inner eyelid ligament (canthus). The tendon is passed through the tunnel, then anchored to the upper and outer portion of the bony orbit.
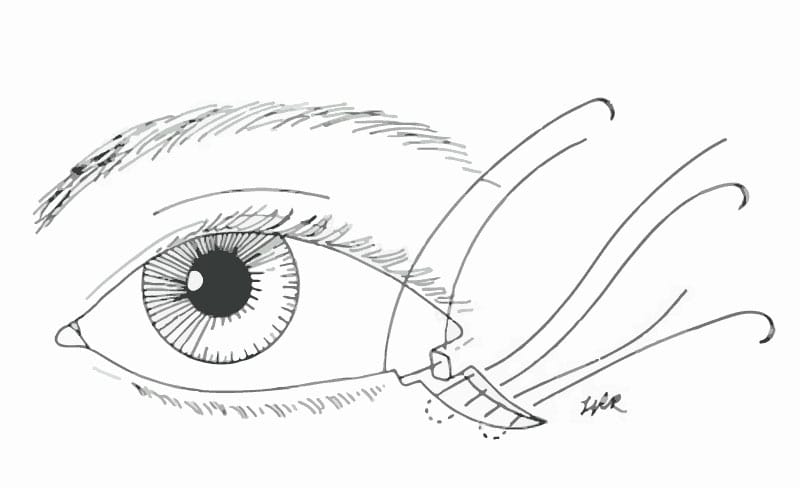
Modified tarsorrhaphy: small incisions are placed along the outer 4-6 mm of the upper and lower eyelids at the margin. The incisions are placed asymmetrically in order to advance the lower eyelid out towards the corner more than the upper eyelid. The incisions are closed with absorbable sutures.
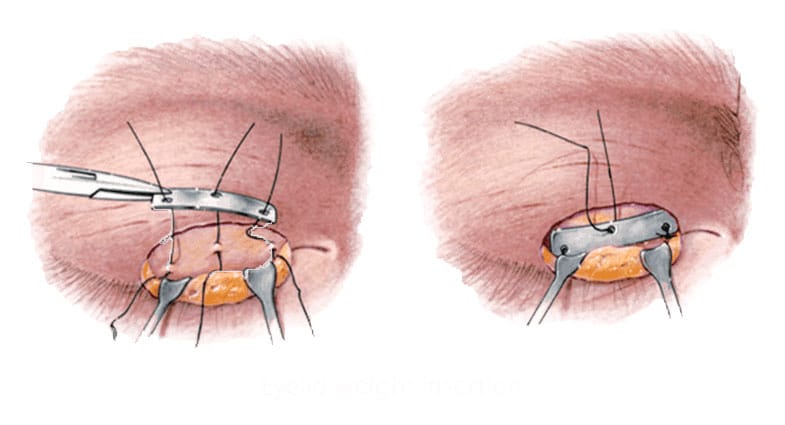
Tarsal wedge resection: also known as lower lid shortening, this involves excising a full-thickness segment of the outer lower eyelid including skin, conjunctivae, and cartilage. The wedge is then closed, tightening up the lower eyelid and slightly elevating it.
Other options are available for both upper and lower eyelid reconstruction in the setting of facial paralysis. Dr. Panossian can go over individual options and tailor the treatment plan accordingly.