
Congenital facial paralysis refers to facial nerve dysfunction present from birth. The condition can result from underdevelopment or complete absence of the facial nerve, affecting one or both sides of the face. It may occur as an isolated condition or as part of broader syndromes such as Moebius syndrome or hemifacial microsomia.
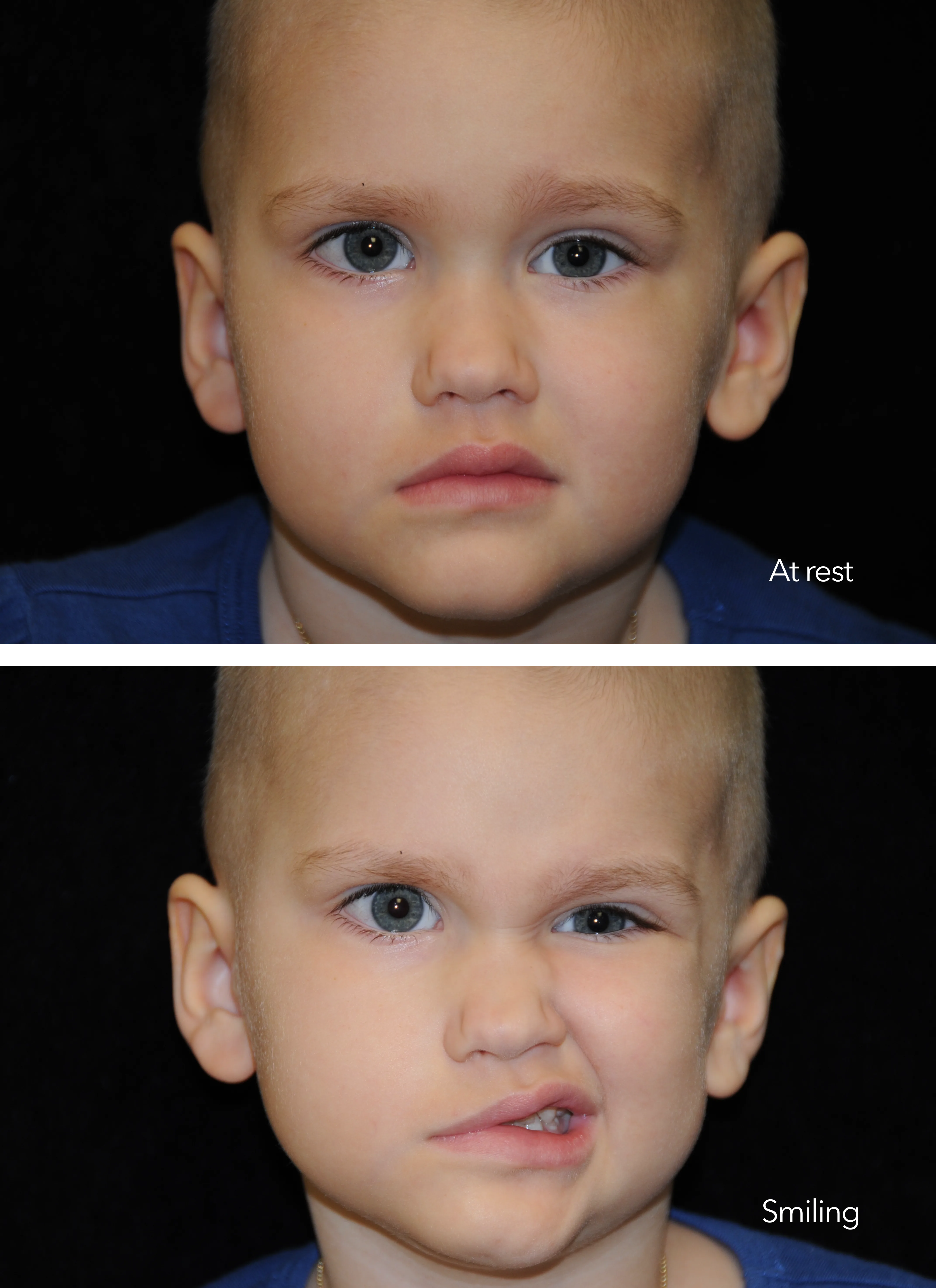
Children born with congenital facial paralysis face unique challenges that extend beyond physical appearance. The inability to smile affects social interaction, emotional development, self-image, and the ability to communicate nonverbally — all critical aspects of childhood development.
Treating facial paralysis in children requires a distinct approach. Their nerves and muscles are still developing, which creates both unique challenges and remarkable opportunities for recovery. Early intervention can be transformative.
Congenital facial paralysis can arise from several causes, each requiring a tailored approach to treatment.

The face can be broken into three key areas of facial nerve function and expression. The upper third deals with forehead elevation. The middle third focuses on eyelid closure. And the primary function of the lower third is dynamic smile and mouth movement. Congenital facial paralysis can impact one or all of these zones.
With paralysis of the forehead, the ability to raise the brow or create wrinkles is affected. People with forehead paralysis are not necessarily noticed right away. However, with animation and simple gestures, the lack of movement becomes obvious. Sometimes, forehead paralysis may result in gradual drooping over the upper eyelid. This can worsen over time and can even partially block vision.
Although a paralyzed forehead may mimic a "permanent Botox®" effect, many people don't care for the look, especially when only one half of the forehead is affected. For those wishing to have a more uniform appearance, Botox® injections to the unaffected side may produce the desired appearance. However, these injections may be required every 3 to 6 months to maintain the effect.
Another option may be to permanently paralyze the normal side of the forehead with a surgical procedure. For patients experiencing problems with their vision due to a heavy, droopy forehead, a brow lift will restore the height of the brow to a desirable level. Dr. Panossian has studied and refined these techniques over many years.


Paralysis of the eyes and eyelids can result in a number of problems. The most serious problem is the inability to close the eye, which can remain open while sleeping. Persistent problems with eye closure may lead to drying of the cornea. In turn, this may result in permanent scarring and eventual blindness. This is the most compelling reason to treat facial paralysis.
Other problems include the appearance of the droopy lower eyelid. Initially, the droop may be subtle, but with time, the lower eyelid will fall further, causing a noticeable deformity. The upper eyelid may also have trouble doing its part to close the eye. Lastly, the dynamic effect of blinking can be affected — typically one of the most difficult functions to restore.
Several solutions exist for the variety of problems that can affect the eye in facial paralysis. The decision to pursue surgery is made in conjunction with an ophthalmologist's evaluation. If signs of corneal scarring (keratopathy) are present despite aggressive lubrication regimens, then the decision to undergo surgery is made urgently.
A number of surgical techniques are available to correct eyelid paralysis depending upon severity. These include placement of an upper eyelid weight, lower eyelid tendon sling, or tarsorrhaphy (suturing outer part of upper and lower eyelids together), among others.
Your child's smile is one of the most unique characteristics about their face. Losing the ability to smile can have profound effects on the ability to socially interact with others, communicate, and develop one's self-image.
Numerous options are available for patients requiring reconstruction. Generally, these options could be categorized as "static" or "dynamic" in nature. Static reconstructions involve resuspending the corner of the mouth in a natural position to counteract the droop of the paralyzed face. This can be done in a number of ways using several natural and artificial options.
Dynamic reconstructions involve the use of techniques to re-establish muscle control of the paralyzed face. This typically involves the transfer of a muscle from another part of the body to the face where it is reconnected to a new blood supply and plugged into a functioning nerve. Over time, the new muscle gains the ability to move and re-activate the lost smile.
Dr. Panossian has developed a new take on an old technique (the Labbé technique) designed to reanimate the smile using a muscle for biting. This muscle, called the temporalis, is one of four muscles used in biting and is located on the side of the head. Dr. Panossian's modifications have improved the time to reanimation and overall patient satisfaction.
Synkinesis is the involuntary movement of facial muscles that can occur after recovery of the facial nerve. This happens most often in the setting of Bell's palsy and can be quite disconcerting for patients. It is the result of miswiring of the downstream branches of the facial nerve during the process of nerve regeneration.
In the setting of facial paralysis, eyelid twitching may be triggered by voluntary activation of other facial muscles, such as smiling or moving the mouth. Treatment to correct this problem can include surgical denervation of the interconnections between the involved muscles or with use of Botox®. Whether mild or severe, correction of eyelid problems is an important part of any treatment plan for facial paralysis.
Dr. Panossian's craniofacial training gives him specialized expertise in pediatric facial reconstruction — understanding not just the surgery itself, but how growth and development affect long-term outcomes.
The gracilis muscle from the inner thigh is transplanted to the face and connected to a functioning nerve — typically the masseteric nerve or a previously placed cross-face nerve graft. When performed in childhood, the transplanted muscle grows with the child, and the brain develops new neural pathways to control it. Results improve over time as the child's nervous system adapts. This is the primary dynamic reconstruction for creating a smile in children with congenital paralysis.
Learn More →Dr. Panossian's refined technique repositions the temporalis muscle — already present and functioning — to power a smile. The muscle becomes functional for smiling within days of surgery, and over time, begins to move spontaneously when the child tries to smile. This single-stage approach offers minimal scars, reduced cheek bulk, and faster results compared to multi-stage procedures. It can be performed in an outpatient setting for most patients.
Learn More →For children with unilateral paralysis, a cross-face nerve graft connects the functioning facial nerve on the healthy side to the paralyzed side using a nerve from the leg. This creates a pathway for spontaneous, emotion-driven movement. Nerve transfers redirect other functioning nerves (such as the masseteric nerve) to power facial muscles. These techniques are often the first stage of a two-stage reconstruction.
Learn More →Protecting the eye is paramount in congenital facial paralysis. Options include upper eyelid weight placement, lower eyelid tendon slings, and tarsorrhaphy. If signs of corneal scarring are present despite lubrication, surgery is pursued urgently. Dr. Panossian also offers corneal neurotization to restore sensation and the protective blink reflex.
Static reconstructions suspend the corner of the mouth in a natural position using fascia slings, counteracting the droop of the paralyzed face. Brow lifts, BOTOX® to the unaffected side for symmetry, and other adjunctive procedures complement dynamic reconstructions. These are tailored to each child's specific needs and developmental stage.
Browse real patient outcomes from Dr. Panossian's facial reanimation procedures.
Treating congenital facial paralysis requires a surgeon with deep understanding of both facial nerve reconstruction and pediatric craniofacial surgery. Dr. Panossian brings both — with fellowship training at Harvard Medical School and the Hospital for Sick Children in Toronto under Dr. Ron Zuker, a global pioneer in pediatric facial reanimation.
Dr. Panossian and his team work closely with families throughout the process, providing guidance on timing, expectations, and the emotional aspects of treatment. He understands that for a parent, the decision to pursue surgery for their child is deeply personal — and he approaches every case with both surgical precision and genuine compassion.
Through his work with Mending Kids, Dr. Panossian has extended this care to children around the world who would otherwise have no access to reconstructive surgery — bringing the gift of a smile to those who need it most.
The timing of facial reanimation depends on the specific procedure and the child's condition. In general, surgical interventions for congenital facial paralysis typically begin around age five, when the child's facial structures have developed sufficiently to support reconstruction. However, eye protection procedures may be performed earlier if corneal health is at risk. Dr. Panossian evaluates each child individually to determine the optimal timing — early evaluation helps families plan ahead even if surgery is not yet appropriate.
Static reconstruction uses tissue grafts (such as fascia slings) to suspend the corner of the mouth in a natural resting position, improving facial symmetry at rest but without active movement. Dynamic reconstruction restores actual muscle movement — the ability to smile voluntarily or spontaneously. Dynamic options include gracilis free muscle transfer (transplanting a muscle from the thigh to the face) and Dr. Panossian's lengthening temporalis myoplasty (LTM), which repositions an existing muscle to power a smile. Many treatment plans combine both static and dynamic approaches for comprehensive results.
Recovery varies by procedure. The LTM technique provides immediate movement on the operating table, with most children returning to normal activities within 2–3 weeks. Gracilis free muscle transfer requires a longer recovery — the transplanted muscle typically begins to show movement at 3–6 months, with continued improvement over 6–12 months as the nerve regenerates and the brain develops new pathways to control the muscle. Dr. Panossian provides detailed postoperative care plans including physical therapy protocols to optimize each child's recovery.
It depends on the severity and extent of the paralysis. Some children achieve excellent results with a single procedure, such as the LTM. Others — particularly those with complete facial paralysis affecting the forehead, eyes, and smile — may benefit from a staged approach that addresses each area over time. Cross-face nerve grafting followed by gracilis muscle transfer is a two-stage protocol. Dr. Panossian discusses the full treatment plan during consultation so families can understand the timeline and set realistic expectations from the beginning.
If your child was born with facial paralysis, schedule a consultation with Dr. Panossian to discuss the options available. Early evaluation helps determine the optimal timing for intervention. In-person and virtual consultations are available.
Request a Consultation