
The gracilis free muscle transfer is the definitive procedure for restoring smile function in patients with long-standing facial paralysis — those whose native facial muscles have atrophied beyond the point of recovery. When paralysis has persisted for more than approximately 18 months, the original muscles of facial expression can no longer be reinnervated. A new muscle must be brought in.
The gracilis — a slender, expendable muscle from the inner thigh — is transplanted to the face using microsurgical techniques. Its blood supply is connected to facial vessels to keep it alive, and its nerve is connected to a motor source that will power it: either a matured cross-face nerve graft (for spontaneous, emotion-driven smiling) or the masseteric nerve (for strong, volitional smiling). Over the following months, nerve fibers grow into the transplanted muscle, and it begins to contract — producing a smile.
The choice of nerve source is one of the most important decisions in gracilis free muscle transfer. Each approach has distinct advantages, and Dr. Panossian helps every patient understand the trade-offs to make the right choice for their situation.
Stage 1: A sural nerve graft is harvested from the lower leg and microsurgically connected from a functioning facial nerve branch on the healthy side, tunneled across the upper lip, and banked on the paralyzed side. Over 6 to 12 months, nerve fibers from the healthy facial nerve regenerate through this graft.
Stage 2: Once the cross-face nerve graft has matured and is carrying a viable neural signal, the gracilis muscle is transplanted to the face. Its nerve is connected to the matured graft, and its blood vessels are connected to the facial artery and vein using microsurgical technique.
The Advantage: Because the motor signal originates from the patient's own facial nerve on the healthy side, the resulting smile is spontaneous — it occurs naturally with emotion, without conscious effort. Patients smile when they feel happy, laugh at a joke, or greet a loved one. No retraining is required.
The Trade-off: This is a two-stage process requiring two separate surgeries spaced 6 to 12 months apart. The overall timeline from first surgery to functional smile is longer than the masseteric approach.
In this single-stage approach, the gracilis muscle is transplanted and its nerve is connected directly to the masseteric nerve — the motor nerve that powers jaw clenching. There is no need for a prior cross-face nerve graft; the entire reconstruction is completed in one operation.
The Advantage: Faster results. Because the masseteric nerve is immediately available and provides a strong motor signal, patients typically see the first signs of muscle contraction within three to four months. The smile produced is powerful and reliable.
The Trade-off: The smile is initially activated by gently clenching the teeth, since the motor signal comes from the bite nerve rather than the facial nerve. With practice and physical therapy, this activation becomes more automatic. Many patients develop some spontaneity over time through cortical adaptation, but the degree of emotional spontaneity is generally less than with the cross-face approach.
The gracilis is one of the most versatile muscles in reconstructive microsurgery, and there is a good reason it has become the gold standard for facial reanimation worldwide.

Gracilis free muscle transfer is among the most technically complex procedures in plastic surgery, requiring expertise in microsurgery, facial anatomy, and aesthetic judgment.
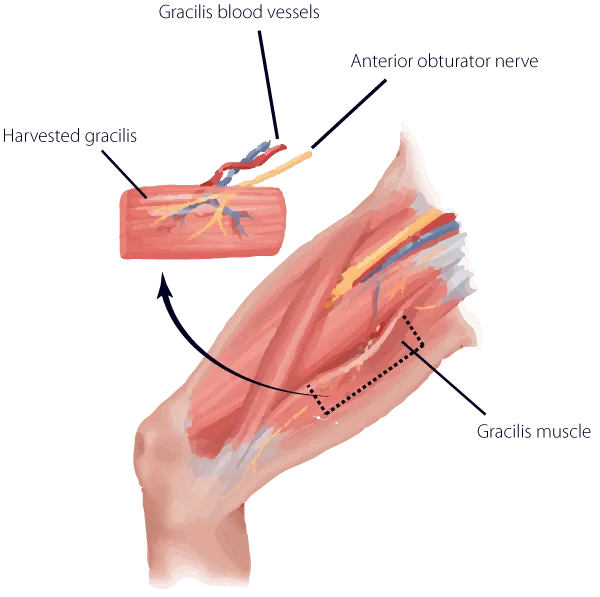
Through an incision on the inner thigh, Dr. Panossian carefully harvests a segment of the gracilis muscle along with its artery, vein, and nerve (the neurovascular pedicle). Only the portion needed is taken — the muscle is tailored to the precise dimensions required for the facial reconstruction. The thigh incision is closed in layers and heals with a thin scar concealed on the inner leg.
On the paralyzed side of the face, Dr. Panossian creates a pocket in the cheek to receive the transplanted muscle. The facial artery and vein are prepared for microsurgical connection. If a cross-face nerve graft was placed during a prior first-stage surgery, its banked end is identified and prepared. If a masseteric nerve approach is being used, the masseteric nerve is dissected and prepared for coaptation.
The gracilis muscle is positioned in the face, anchored at the oral commissure (corner of the mouth) on one end and the zygomatic arch (cheekbone) on the other — replicating the vector of a natural smile. Under the operating microscope, the muscle's artery and vein are connected to the facial vessels using sutures finer than a human hair. The muscle's nerve is then connected to the chosen motor source. Blood flow is confirmed, and the muscle is secured in its new position.
The muscle's bulk, tension, and vector are carefully calibrated to produce a natural-appearing smile that matches the healthy side as closely as possible. This step requires equal parts surgical skill and aesthetic judgment — the difference between a technically successful transfer and a beautiful result often comes down to these fine adjustments. Dr. Panossian's dual expertise in reconstructive and aesthetic surgery is particularly valuable here.
Gracilis free muscle transfer is a major microsurgical procedure, and patients should understand both the potential benefits and the risks involved. Dr. Panossian discusses these thoroughly during the consultation process.
While the goal is symmetric movement, the transplanted muscle may produce a smile that differs slightly in timing, strength, or excursion compared to the healthy side. Some patients experience cheek fullness or a subtle contour difference from the underlying muscle bulk. Dimpling at the attachment points is possible. The nasolabial fold on the reconstructed side may not perfectly match the other side. Many of these issues can be refined with secondary procedures if desired.
In a small percentage of cases, the microsurgical connections to the muscle's blood supply may not remain patent, resulting in partial or complete muscle loss. This is the most serious complication and may require a second transplant. Dr. Panossian's extensive microsurgical experience minimizes this risk, and patients are monitored closely in the immediate postoperative period for any signs of vascular compromise.
The degree of nerve regeneration into the transplanted muscle is not entirely predictable. Some patients achieve strong, full-excursion smiles while others develop more modest movement. Factors including the quality of the nerve source, the patient's age, and overall health all influence the outcome. Physical therapy plays a critical role in maximizing whatever innervation is achieved.
As with any surgery under general anesthesia, there are standard risks of bleeding, infection, hematoma, and anesthesia-related complications. These risks are relatively low and are managed through careful preoperative planning, sterile technique, and postoperative monitoring.
Recovery from gracilis free muscle transfer requires patience, but the results — the return of a genuine smile — are transformative for patients who have lived without one.
Weeks 1–3: Restricted activity and a soft diet protect the microsurgical connections and muscle positioning. Swelling and bruising are expected and gradually resolve. The thigh donor site heals with routine wound care.
Months 3–6: The first signs of muscle contraction typically appear as nerve fibers grow into the transplanted gracilis. With a masseteric nerve source, movement may appear as early as three months. With a cross-face nerve graft, it may take four to six months. Early movement is often subtle — a twitch or flicker — that progressively strengthens.
Months 6–18: The smile strengthens and becomes more refined. Physical therapy is essential during this phase, helping patients develop control, coordination, and natural-appearing movement. The muscle may undergo some initial bulkiness that softens over time as it adapts to its new function.
Beyond 18 Months: The result is considered mature. Secondary refinements — such as debulking, scar revision, or symmetry adjustments — can be performed if desired. Many patients require no additional procedures.
Gracilis free muscle transfer for facial reanimation is one of the most technically demanding operations in all of plastic surgery. It requires mastery of microsurgical technique — connecting vessels and nerves smaller than a millimeter in diameter — combined with a nuanced understanding of facial anatomy, aesthetics, and the biomechanics of smiling. The surgeon must simultaneously think like a microsurgeon, a facial specialist, and an artist.
Dr. Andre Panossian trained specifically in this procedure under Dr. Ron Zuker at the Hospital for Sick Children in Toronto — the institution where the modern technique of gracilis free muscle transfer for facial reanimation was pioneered and refined. This mentorship, combined with his craniofacial fellowship at Harvard Medical School, gives him a depth of expertise that few surgeons in the world can match.
His featured role on the TLC series "About Face" has showcased this procedure to a broad audience, but the cases that matter most are the ones that happen quietly — in the operating room and in follow-up visits where patients see their smile return for the first time. For Dr. Panossian, every gracilis transfer represents a profound commitment to restoring something fundamentally human: the ability to express joy.
No. The gracilis is a redundant muscle — other muscles in the inner thigh compensate fully for its absence. Patients experience no meaningful weakness in their leg, and even athletes return to full activity. The donor site scar is on the inner thigh and easily concealed by clothing.
The cross-face nerve graft approach produces the most natural, spontaneous smile but requires two surgeries and a longer overall timeline. The masseteric approach is a single surgery with faster results but initially requires conscious activation to smile. Your age, goals, timeline, and clinical anatomy all factor into this decision. Dr. Panossian discusses both options in detail during consultation and recommends the approach that best aligns with each patient's individual priorities.
The first signs of muscle movement typically appear three to six months after the gracilis transfer, depending on the nerve source used. The smile continues to strengthen and refine over 12 to 18 months. For patients undergoing the two-stage cross-face approach, add 6 to 12 months for the initial nerve graft maturation. While the timeline requires patience, the result — a genuine, functional smile — is one of the most rewarding outcomes in all of surgery.
Complete flap failure — where the muscle does not survive the transfer — is rare but possible, occurring in a small percentage of cases. If this happens, the procedure can typically be repeated with a gracilis from the other thigh. Incomplete innervation (where the muscle survives but produces less movement than expected) is more common and can often be addressed with physical therapy optimization or secondary procedures. Dr. Panossian sets realistic expectations during consultation and monitors every patient closely throughout their recovery.
If you've been living with facial paralysis and are ready to explore the possibility of smiling again, the gracilis free muscle transfer may be the answer. Schedule a consultation with Dr. Panossian to discuss your options and begin your journey toward restored expression.
Request a Consultation